Runes for health promotion. Treatment of hypertension runes ruffeed
 Live Journal
Live Journal Facebook.
Facebook. Twitter.
Twitter.In the given work, on the basis of these modern literature, the main physiological and pathophysiological aspects of the PCF measurement are presented, testimony for monitoring of the ICF and its clinical significance.
Introduction
Treatment of patients with sharp cerebral damage almost always represents a serious problem and, above all, due to the peculiarities of the intracranial system located in a closed hermetic cavity of the skull with a fixed volume. Pathogenesis and tanatogenesis of patients with cerebral damage has been studied quite fully. The result of this study unequivocally showed the leading role of acute intracranial hypertension syndrome (VCH). The importance of a quantitative assessment of the values \u200b\u200bof pressure in the cavity of the skull for patients with cerebral pathology is currently no doubt. Moreover, humanity has passed a certain way and in a methodological aspect, developing various methods for measuring VCHD. This work is devoted primarily to such as aspects as a methodology for measuring ICF and its clinical value.
History of measurement of the GFD.
The first attempt to measure intracranial pressure (VCHD) by the method of lumbar puncture produced in 1897 Quincke. The first directional neurosurgical intervention according to the results of the measurement of the HBD was performed by Sharpe W. in 1920. The author has determined the testimony for the performance of omissant decompressive cranectomy in the development of intracranial hypertension.
At the beginning of the 20th century, many clinicians were measured by the PCD with lumbar puncture and used the indicators of liquor pressure for the diagnosis of intracranial hypertension and as a reference point for subsequent therapy. At the same time, discrepancies between the clinic of the disease and the indicators of the likvorn pressure were noted. So in some cases, dislocation symptoms or an intracranial hypertension clinic was recorded in the absence of high values \u200b\u200bof liquor pressure in the lumbachal space.
An explanation of this phenomenon gave Langfitt in 1964. He conducted simultaneous registration of pressure in lumbar and intracranial spaces and set the pressure difference in two spaces. Langfitt noted the existence of a pressure gradient between the liquor spaces in the presence of volumetric formation above or below the brazower outline, which causes compression of the likvorn paths. Langfitt found that the method has a clear limitation and it must be considered: the permeability of the likvorn should be preserved.
The first continuous measurement of the PIRE (monitoring) produced Pierre Janny in 1950. However, his work was published only in 1972. Therefore, Nils Lundberg is considered a pioneer in the monitoring of the HCD, which in 1960 published his work "Continuous Recording and Control of Ventricular Fluid Pressure in Neurrosurgical Practice". Analyzing the trends of the CHD, Lundberg allocated different types of Wasters of the VGD: A, B, and C - waves. The most significant waves that we encounter in our practice is a - waves or plateau waves. The name of the wave was obtained for a characteristic form. A - waves reach the amplitude to 50 - 100 mm Hg. And there are a duration of 5 minutes and more. Plate waves are formed during the dilatation of cerebral vessels of the brain. The main cause of this phenomenon can be a decrease in cerebral perfusion pressure, reduction of systemic blood pressure or hypercap. Plate waves are accompanied by a critical reduction in cerebral-perfusion pressure (CPD), which can cause brain ischemia. It has been proven that the appearance of plateau waves indicates the preserved cerebral auto regulation and is an indicator of reduced elasticity (elastance) of the brain. Since plate-waves are formed only in the presence of brain vessels, it is enough to carry out hyperventilation and run a vasoconstrictor cascade, raising the Hell and CPD.
Waves in and with do not have an important clinical value. B - waves can be transformed into a plateau wave. The study of Castellani G. and Sovat showed that the plateau waves are more often recorded in the victims of young age, more often with CHHMT closed, the minimum volume of contusion focus, a small lateral dislocation of the median structures according to computer tomography (CT). . According to the conclusions of the authors group, the presence of plate-waves at CMT is a prognostically favorable sign, as it indicates the safety of the anti-self-regulation of cerebral vessels. It is important to remember that the plateau waves must be immediately eliminated due to the risk of developing cerebral ischemia. Plotophysiological aspects of the measurement of the GFD.
The measurement of the ICD is based on the monro-kelly doctrine, which reads: - All intracranial volumes are enclosed in a rigid bone formation - the skull cavity and the total volume of intracranial components (blood, liquor and brainstatus) remain constant; - when the additional volumetric component appears (tumor, hematoma, swelling) or changes in the volume of any of the above three, the total volume should remain unchanged; - Volume equilibrium between the components of the intracranial system ensures the constancy of the pressure in the skull cavity. In other words, compensation of the increase in the volume of one of the components should be provided with a proportional decrease in the volume of one or two other components. Intracranial components providing volumetric equilibrium are the liquor and the venous component of intracranial blood volume. Violation of volumetric equilibrium leads to an increase in PCF. The diagnostic value of the measurement of the ICF is that it allows to judge the state of volumetric compensation in the cavity of the skull. Mathematically, the monro-kelly doctrine can be expressed by the formula: V \u003d VKrov + VKRVOR + VINKOMG, orV \u003d ΔVPAT +. ΔVKrov + ΔVerkvor + ΔVMind, where V is the total volume of blood, ΔV is a change in the volume of intracranial components.
Monroe - Kelly doctrine can be sketchically presented (Fig. 1 - Monro-Kelly Doctrine Scheme. Intracaranteed Content: Brainstatus, Blood, Likvor.). The brain substance is 80-85% intracranial volume or 1200-1600 ml: neurons 500-700 ml, GLAY 700-900 ml, extracellular liquid up to 75 ml. Blood and liquor total constitute 15-20% intracranial volume, i.e. Approximately 100-150 ml.
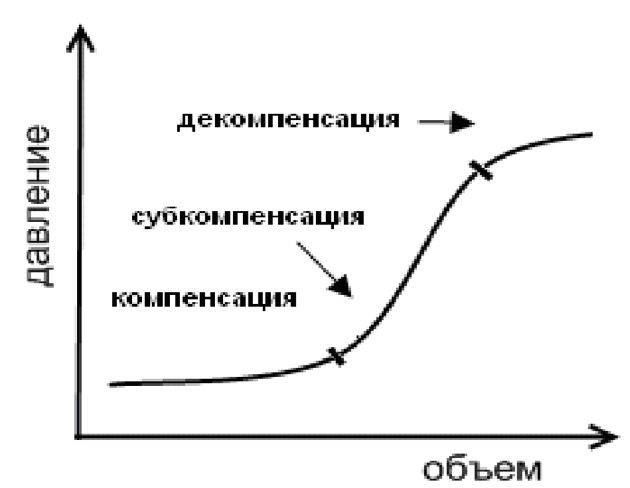
The relationship of intracranial volumes in the skull cavity can be represented graphically curve volume - pressure (Fig. 2. Curve Relationship Currency Volume: Stages of compensation, subcompensation and decompensation.). The graph is an exponential curve. It highlights a common part, which characterizes the zone of volumetric compensation. In this section of the graph, any increase in intracranial content does not lead to an increase in the ICD, as the liquor and venous compensation mechanisms are triggered. However, the possibilities of compensatory mechanisms are not limitless and followed by a gentle part should be the sharper part of the exhibitory. In this area, the minimum increase in intracranial volume (hematoma, edema, etc.) leads to a sharp increase in pressure and development of intracranial hypertension. In clinical practice at this point, we register a drop in perfusion pressure, an increase in the PCF and the appearance of plateau waves. Ertianized events will not be adopted at this stage of the pathological process, the next phase of severe disorders comes with the formation of ischemia, dislocation and brain deploying.
It is important to remember that patients with cerebral pathology are often located in this transition zone and have a reduced reserve of volumetric compensation. Often these patients have the oppression of the level of consciousness (Sopor, Coma), are located on an extended IVL and receive sedative therapy. All this makes it difficult to adequate clinical and neurological assessment in the dynamics. The development of the decompensation phase in this category of patients can occur imperceptibly and fast enough. With such clinical situations, monitoring of the CFD makes it possible to diagnose the development of intracranial hypertension and assess the level of compensatory mechanisms.
What is the VGD?
The single definition of the HBD is not strange, but does not exist. According to the monro-kelly doctrine, this is a certain uniformly distributed pressure inside the cavity of the skull.
There are other definitions of the HCD, for example: ... This is the pressure of the cohadon f et al. 1974 ... Pressure in the cortical veins and venous sinuses Johnston H. et al, 1974 ... Pressure of the liquor in the ventricles of the brain Lundberg N. 1960 The DAVSON equation describes the GFD as the pressure of the spindy fluid, which depends on the speed of the production of liquor, the resistance of the outflow of liquor and pressure in the Sagittal venous Sinus: ICP \u003d CSF Pressure \u003d Resistance CSF Outflow x Rate CSF Outflow + P Sagittal Sinus, where ICP - intracranial pressure, Resistance CSF Outflow - Faculture Otte Resistance, RATE CSF Outflow - Liquor Protect speed, P Sagittal Sinus - Venous pressure in Sagittal Sine .
However, only the likvorn pressure cannot determine the GFD. According to the mathematical model, which was described by Marmarou A. et al., In addition to the likvorn component, an important component in the formation of the CFF is a "vasogenic" or vascular component. According to the author, it is the vascular ("vasogenic") component plays a decisive role in the formation of intracranial hypertension in patients with traumatic height of the brain. On the author, according to the author, there is only a third part in the development of intracranial hypertension. The main "vasogenic" mechanisms that define the GFD are: blood pressure, venous outflow, and the autoregulation of cerebral vessels.
It is well known that both arterial hypertension and arterial hypotension can lead to intracranial hypertension and brain edema due to the formation of hyperemia or ischemia. The difficulty of venous outflow leads to an increase in the blood flow of the brain and, ultimately, to the development of cerebral edema. The loss of auto regulation can contribute to the formation of brain edema, both in the development of hyperemia and under ischemia.
VCHD in normal
Normal Values \u200b\u200bof the HBD may vary depending on age, body position, and clinical condition. In an adult man in a state of rest on the back of the HBD ranges from 5 to 15 mm Hg, and in the standing position can take a negative value to - 5, and in the presence of the shunting system, it is not enough to be lower than - 15 mm Hg. . In childhood, it is a value of 3 to 7 mm Hg, and in the newborn it ranging from 1.5 to 6 mm Hg.
The value of the value of the VEC is over 15-18 mm Hg. It is considered a pathological condition. The testimony for treatment at hydrocephalus is the VCHD above 15 mm Hg., And at the THMT above 20 mm Hg. .
Methods of registration of the PCD.
Methods for measuring the PCD can be divided conditionally depending on the location of the GFF sensor (Fig. 3 Methods for measuring VFF, depending on the location of the sensor:
- subdural
- parenchimato
- ventricular
- epidural
- subarachnoidal
- solid brain shell
- side stomach brain

The most early method and preserving the right to be called "golden" standard is considered to measure the liquor pressure in the cavity of the brain side ventricles.
Ventricular measurement of the PC.
For ventricular measurement of the HBD at the point of the Kohiber, ventriculostomy is performed. The measurement of the liquor ventricular pressure is carried out with the help of a strain gauge sensor, which is hosted extra at the level of the outer auditory. It is this position of the transdewsser that provides a zero value of the ICF, which corresponds to the anatomical projection of the mono hole. This method of measuring GFD remains reference from the time of work Lundberg. The method does not require expensive equipment, easy to use and interpret data. The method has its advantages and disadvantages.
The advantages of the ventricular measurement of the GFD: remains the cheapest and affordable.
The method makes it possible to recalibrate the sensor in the development of the "zero drift". It also makes it possible to analyze the liquor on cellular and biochemical composition, perform metabolic and bacteriological monitoring. The method is not only diagnostic, but also therapeutic, as it allows you to control the CFD by draining the liquor to the disadvantages of the method can be attributed: the risk of developing infectious (5%) and hemorrhagic complications (1.1%) The likelihood of technical difficulties in the fulfillment of ventriculostra Brain and narrowed side ventricles.

Compliance with asepsifetics and antiseptics, antibacterial prevention, use of closed systems for ventricular drainage (Fig. 4 System of external ventricular drainage CODMAN EDS 3 TM. 1 - Measuring line, 2 - air filter of the accumulative tank, 3-tank, 4 - measuring channel for connecting outdoor A strain gauge sensor, 5 - three - chassis for measuring VCHD and drainage of liquor, 6 is a three-chassing crane for liquor drain.), antibacterial coating catheters reduces infectious complications.
Other invasive methods for measuring VCHD.
To date, it is believed that the measurements of the HBF in subdural and subarachnoid spaces are less accurately compared with the parenchymal and ventricular dimension. All attempts to introduce new techniques pursued the only goal - to reduce the likelihood of infectious and hemorrhagic complications, as well as simplify the method for installing the GUL sensor. From these positions, a very encouraging method was the method of epidural location of the GCH sensor. However, intracranial pressure indicators in epidural measurement are strongly overlapped in comparison with the lumbar and subdural dimension.
There were attempts to measure the PCF in the lumbar space, or rather the measurement of the liquor pressure. The given methodology, as discussed earlier, had its limitations due to the inaccuracies of measurement in the presence of the compression of the liquor-conducting paths. It must be remembered that the lumbar puncture at the edema of the brain can cause axial dislocation and the penetration of the brain. . In modern recommendations for children's neurotramatology, drainage of the lumbar space is allowed, as an additional option when the unguided intracranial hypertension is stopped (HFG). The method is considered as a method that increases the reserve of craniospinal space. There is experience in using auxiliary lumbal drainage with an unknown RFG in patients with CMT and SAC. The authors make a reservation that lumbal drainage can only be used in the passability of the liquor-conducting pathways and the absence of the block at the level of the covering tank. Modern technologies make it possible to simultaneously carry out continuous measurement and controlled drainage of the liquor with strict control of the specified level of liquor pressure, not allowing the development of hyperaening and brain dislocation. Such capabilities have the LiquoGuRard system (Moller Medical GmbH @ Co.KG), which allows to carry out controlled drainage of the liquor within the specified values \u200b\u200bof the likvorn pressure.
Among invasive techniques, the most common parenchymal measurement method remains. The sensor is installed in a cerebral parenchyma to a depth of 2-2.5 cm. The sensor is installed through a triferization hole at the point of Kochra, which is used when puncture of the front horns of the side ventricle. The PWC sensor can be fixed using a special bolt-system (Richmond Bolt) or with preliminary tunnel under the skin. The sensor is implanted in the premotional zone of the non-general hemisphere. The parenchymal method of measuring the HCB is considered preferable, since it is better than the remaining methods corresponds to the testimony of intraventricular measurement. The disadvantage of the parenchymathous measurement of the PCF is the high cost of the sensor and the impossibility of recalibration, the need to which occurs during the "zero drift".
Non-invasive methods for measuring VCHD
The literature covered various ways of invasive and non-invasive assessment of the PCF. Searches more accurate and easily playable method continue. The relevance of the development of new non-invasive techniques is dictated, first of all, an attempt to minimize all complications associated with invasive measurement of the PCF. In addition, individual patients and in certain age groups, such as newborns, babies, people of old age, as well as in patients with hemostasis impaired, the use of non-invasive measurement methods is obviously preferable.
In the special literature, the possibility of assessing the ICF on the displacement of the eardrum is discussed. It is assumed that the change in the CFD changes the pressure of the perilimphs in the snail maze, and this leads to a displacement (deformation) of the eardrum. However, this technique is described only for patients with hydrocephalus. The prerequisite for the use of this technique is the preservation of the structures of the middle ear and the brain barrel. According to the authors, the measurement result is a surrogate marker of the GFD and can serve only as an estimated indicator reflecting the dynamics of the CFC change in a particular patient. The method requires further improvement and cannot yet be recommended for widespread use.
One of the attempts to evaluate the PCF and the CPD was an interpretation using dopplerography. To calculate the CPD, a computer analysis of the wave characteristics of blood pressure and linear blood flow rate is used. The method allows for measuring the CPD with the error of +/- 10 mm Hg.
Studies were conducted on the measurement of the PCF using ophthalmodinamometry. The method has proven itself as inaccurate and gave large errors in patients in a coma and with myopia. The method of quantitative poinometry, the essence of which is to estimate the speed of papilocontractions, which decreases with the development of intracranial hypertension. The method allows you to identify patients with pronounced hypertension (CBD above 20 mm Hg), but requires the use of special equipment.
The literature covered methods based on estimating the speed of passing an ultrasonic wave in the skull cavity. It is assumed that the rate of passage of the ultrasonic wave will depend on the density of intracranial content, i.e. change in the development of cerebral edema. In patients with CHMT, comparable results of invasive ("Camino") were obtained and an incomparable measurement of the VITTamed sonographic monitor.
Newborn and babies were measured in non-invasive via Fontainnell (unexpressed spring). To this end, a special contact sensor was developed (Rotterdam Teletransducer), which was applied to an unexecuted front spring and fixed on his head with a lightweight frame. The results of monitoring 70 babies, both healthy and various neurological pathology, gave very encouraging results. Further improvement of this technology showed comparability of the RotterDam TeleTransducer sensor readings on infants with hydrocyphalia with an invasive measurement of the PCF, as well as a high degree of correlation of two methods (R \u003d 0.96-0.98).
The development of non-invasive methods for measuring GFD remains relevant. Currently, a leading place occupy various ultrasound and telemetry measurement methods. The question of the accuracy of the data obtained with non-invasive methods remains open and requires further clarification. All of the above methods do not allow to measure the absolute value of the VGD, but only allow you to extrapolate the dynamics of its changes.
Indications for measuring VCHD.
Over the past 15 years, the use of the monitoring of the monitoring is not limited to victims of the CHTMT. The list of diseases in which the measurement of the CBF was carried out significantly expanded: - intracranial hemorrhages and sac - hydrocephalus - stroke, accompanied by edema of the brain - postgoxic encephalopathy - infectious meningitis - hepatic encephalopathy. Indications for conducting invasive measurements of the ICD are clearly established for patients with severe acceleracy injury. First of all, the indication for the monitoring of the CBF is the comatose state and the presence of pathological changes according to CT. The testimony for monitoring of the HFD is also a comatose state in the absence of changes to the CT, but if there are any two of three signs: age over 40 years, post-tonic reactions, systolic blood pressure< 90 mmHg.** Спорные вопросы мониторинга ВЧД.
The development of intracranial hypertension is associated with a high risk of fatal outcome, but there are reports that not all patients with a high HBD have an unfavorable outcome. This is not surprising, since the parameters of the HCD and CPD cannot characterize all pathophysiological processes in the damaged brain and reflect all the variety of cerebral processes. Currently, it is shown that the therapy oriented only on the parameters of the CPF and the CPD in a number of clinical situations is not able to prevent the development of secondary ischemic brain damage. To date, not a single randomized controlled study was conducted, confirming the impact of the monitoring of the monitoring on the outcome of injury. This comparison is not possible for simple ethical considerations. In addition, according to the calculations, to confirm differences in the outcomes between compared groups, significant financial and material costs will be required.
A survey conducted among neurosurgeons and intensivists of different countries has established that the present time does not exist a single approach to the use of various monitoring methods in neurointensive therapy. As for the measurement of the GCH, in the US, the US monitoring was used in 83% of patients with severe CMT, and only 57% of victims were covered in the UK and Ireland. Despite the fact that in Canada there was the highest indicator of the use of the PCF, only 20% of neurosurgeons believe that this method can significantly improve the outcome at the CMT.
A rather "interesting" study conducted a group of authors from Holland, which compared the outcomes and aggressiveness of therapy among victims of severe CMT, who entered in two different medical centers. In the first center was not used by HBD monitoring, and the average blood pressure by all received was provided at a level not lower than 90 mm Hg. In the second center, a protocol focused on providing the CPD above 70 and VCH is below 20 mm RT. Art. The conclusion made by the authors was very unexpected. The therapy focused on the VCD / CPD protocol leads to an increase in the duration of artificial ventilation of the lungs and increases the aggressiveness of therapy, without improving the outcomes. Work is often cited on the pages of special literature devoted to the problem of monitoring the PCF. This publication contradicts most reports on the value of the measurement of the PCF. It is often used as a counter-argument in discussions on this issue, but at the same time is an argument in favor of holding a prospective study that could resolve disputes around monitoring of the PCF.
Gradients of pressure in the skull cavity.
The unevenness of the distribution of values \u200b\u200bof the GFF in the skull cavity is currently a generally recognized fact, but many questions remain unresolved. If the skull cavity was filled with a homogeneous liquid, then the pressure in all points of the intracranial space would be the same. Since the brain is inhomogeneous in composition, its structures (bark, conducting paths, subcortical nuclei, vascular network and liquor spaces) have different density and elasticity. Increased pressure in the damaged zone in each case is redistributed and lines in the cavity of the skull in different ways and in different times. It is obvious that the elasticity of the brain depends on the amount of intra and extracellular fluid in the brain tissue, the state of the vascular system of the brain and blood flow, the presence or absence of atrophy of the brain tissue and the state of the liquor system. Currently, publications devoted to the study of intracranial pressure gradients and the dynamics of the redistribution of GFD, little.
The existence of a gradient of pressure in the skull cavity is higher and below the brain scale was described in the postoperative period in patients undergoing operations to remove tumors in the rear cranial fossa. Rossenwasser et al. It was established that in the HBD in the rear cranial fossa exceeded the value of the GFD in the lumen of the brain ventricles on average by 50%. This gradient persisted in the postoperative period to 12 hours.
With simultaneous bilateral registration of intracranial pressure in subdural space in patients with supra- and infrattorial tumors, the pressure gradient has always been detected between a healthy and affected side.
With sharp subdural hematomas, the simultaneous measurement of the GFF in the parenchyma of both frontal fractions revealed an inter-stroke pressure gradient, which exceeded 10 mm Hg. However, with focal lesions of the substance of the brain and under intracerebic hematomas, the Gradient of the HCD was not registered. According to the authors who carried out this comparative study, the measurement of the PCF with subdural hematomas is advisable to carry out the defeat (ipsilateral).
In clinical work Yano M. et al. The intermetrous gradient was not revealed under various types of traumatic lesions. According to other authors at various intracranial lesions (sheath hematomas, the foci of the injury, etc.) a suprattorial pressure gradient could be quite significant, reaching 20-28 mm RT. St .. Mindermann and Gratz (1998) On a group of patients with TSMT showed that even in the absence of damage to the mass effect, an inter-impassary pressure gradient may develop. The authors argue that the simultaneous 2-third-party measurement of the CFD can be justified in the early period of CHMT, and the control of the CPD with the correction of intracranial hypertension can eliminate this gradient.
When comparing groups with various types of brain damage, it was found that the intermetrous pressure gradient is missing during diffuse damage and appears during focal damage. In case of focal damage, the pressure gradient was allowed for 4 hours and indicated the transformation of the primary focus or the formation of a new focus. An important condition for resolving the pressure gradient, in the opinion of the authors, was the permeability of subarachnoid spaces. The frequency of development of the pressure gradient with focal supratentorial brain damage was 25%. Most of these patients on CT registered the lateral mixing of the median structures.
The most important of the pathophysiological mechanisms leading to the formation of the pressure gradient is considered to be the formation of vasogenic edema in the zone around the tumor or focal brain damage. Against the background of the formation and transformation of primary foci of brain tissue, there are also changes in local brain blood flow, the content of the liquid in the brain substance, the change in the elasticity of the brain - all these dynamic pathophysiological processes also lead to the development of the pressure gradient in the brain substance. A certain contribution to the development of pressure gradient in the edema of the brain introduces a violation of venous outflow, which develops during the obstruction of venous reservoirs against the background of elevated PCF.
In the parenchymal measurement of the GFF, the side of the sensor arrangement depends on the nature of the brain tissue. With focal brain damage, the sensor is located on the side of the pathological focus (hematoma, injury, etc.), with diffuse damage (DPE, diffuse edema, etc.) - the measurement is carried out by the part of the non-dominant hemisphere. The simultaneous measurement of the ICD in different zones (bilateral, infra- and supracentorial, ventricular and lumbal) with different pathology has always demonstrated the presence of a pressure gradient. A number of authors believe that only a small group of patients a multifocal measurement of the HCD can be justified.
The importance of timely diagnosis of pressure gradient is due to the fact that the development of the gradient can lead to the dislocation of the brain structures. The rigidity of the design of the skull, the unevenness of its base with numerous bone protrusions, as well as the presence of the rigging of the solid cerebral shell (Falx, the cerebellum will, etc.), when the brain is dislocation, they determine different types of coupling.
The above review indicates the unevenness of the pressure distribution in the skull cavity. The question of choosing a method for measuring and location of the GUL sensor is important. Modern recommendations on monitoring involve the measurement of only the "global" CBD, with the advantage of the use of ventricular and parenchymal measurement methods. In neurosurgery and neurointensive therapy, making a decision on the tactics of maintenance is always conducted on the basis of a comprehensive patient's assessment, which includes the monitoring of the "global" VCHD, neurovalization methods (CT, MRI), as well as a clinical and neurological assessment.
Arguments in favor of monitoring of the HFD or why it is important to measure the PCD.
Intracranial hypertension occurs in 80% of victims with severe CMT, and a third develops an unmanaged WFG and later they die. In the group of patients with severe CMT, the normal PCD mortality is 17%, and with an increase in the VCHD over 20 mm Hg. reaches 47%.
Intracranial hypertension is a factor of an unfavorable outcome for traumatic brain damage. Prognostic value is not only severity, but also the duration of hypertension. The longer time there is intracranial hypertension, the higher the likelihood of adverse outcome and exit to the vegetative state. It has been established that not only the duration of intracranial hypertension, but also the response to therapy has prognostic value.
Currently, the measurement of the ICD has already been included in the category of routine clinical techniques. The measurement of the PCF is carried out in different categories of patients, both in patients with SAC and CMT and patients after removing brain neoplasms. The monitoring of the CHED allows you to control and control cerebral perfusion pressure (CPD) in patients with complicated passage of the postoperative period, as well as to carry out directional pathogenetic therapy with various cerebral pathology: brain edema, cerebral doubt, etc..
Monitoring of the CHD allows you to evaluate the effectiveness of the anti-edema therapy. It is impossible to carry out therapy without assessing the effectiveness and duration of its effect. Invasive measurement of the CHD makes it possible to measure cerebral perfusion pressure, which reflects the effectiveness of cerebral blood flow and is an independent prognostic indicator. When monitoring the HBD, special software allows you to assess the condition of cerebral autoreguing and brain elasticity. This information is valuable when choosing the therapy tactics. So, on the basis of the estimated coefficient of cerebral reactivity of the brain vessels, the "optimal values" of the CPD can be achieved.
Conclusion
Despite the half-century history of measuring VCHD, the searches and development of new methods for measuring ICF continue. In the treatment of patients with acute cerebral pathology, one of the important tasks remains the treatment of intracranial hypertension. Monitoring intracranial pressure ensures fast and accurate diagnosis of this pathological state and allows you to carry out directional pathogenetic therapy, which favorably affects the outcomes of treatment.
Literature
- Bashkirov M.V., Shakhovich A.R., Lubnin A.Yu. Intracranial pressure and intracranial hypertension. Russian Journal of Anesthesiology and Intensive Therapy 1999; 1: 4-11.
- Belkin A.A., Alasheev A.M., Inyushkin S.N. Transcranial doppler in intensive therapy. Methodological manual for doctors. Ekaterinburg: Edition of the Clinical Institute of the Brain Sunz Ramna; 2004.
- Oshorov A.V., Savin I.A., Goryachev A.S. et al. The first experience of using the monitoring of the anti-tullement of cerebral vessels in the acute period of severe acceleracy injury. Anesthesiology and resuscitation 2008; 2: 16 - 20.
- Flame F., Posner D. Diagnostics of the stupor and coma. Per. from English M.: Medicine; 1986.
- Saribekyan A.S. Transcranial doppler when evaluating the level of intracranial pressure. Journal Neurol. and psychiatrist 1994; 1: 34-37.
- Shakhovich A.R., Shakhovich V.A. Diagnosis of brain circulation disorders (transcranial doppler). M. Medecin; 1996.
- ADELSON PD., BRATTON SL, CARNEY NA. et al. Guidelines for the ACUTE Medical Management of Severe Traumatic Brain Injury in Infants, Children and Adolescents. PediaTr. Crit. Care Med. 2003; (4) 3.
- Andrews P, Citerio G. Intracranial Pressure. Part One: Historical Overview and Basic Concept. INTENSIVE CARE MED. 2004; 30: 1730-1733.
- Asgeirsson B., Grande Po., Nordstrom CH. A New Therapy of Post-Trauma Brain Oedema Based on Haemodynamic Principles for Brain Volume Regulation. INTENSIVE CARE MED. 1994; 20: 260 - 267.
- Balestreri M., Czosnyka M., Hutchinson P., et al. Impact of Intracranial Pressure and Cerebral Perfusion Pressure On Severe Disability and Mortality After Head Injury. Neuroccrit. CARE 2006; 4: 8 - 13.
- Banister K, Chambers IR, Siddique MS, et al. INTRACRANIAL PRESSURE AND CLINICAL STATUS: ASSESSMENT OF TWO INTRACRANIAL PRESSURE TRANSDUCERS. Physiol. Meas. 2000; 21 (4): 473-479.
- Broaddus WC, Pendleton Ga, Delashaw SB, et al. Differential Intracranial Pressure Recording In Patient With Dual Ipsilateral Monitors. In: Hoff JH, Betz Al. (EDS) INTRACRANIAL PRESSURE VII. Berlin, Springer, 1989. 41-44.
- Bundgaard H., Cold GE. Studies of Regional Subdural Pressure Gradients During Craniotomy. Br. J. Neurrosurg. 2000; 14 (3): 229 - 234.
- Castellarani G, Zweifel C, Kim DJ, Carrera E, et al. Plateau Waves in Head Injured Patients Requiring Neurocritical Care. Neuroccrit. CARE 2009; 11 (2): 143-50.
- Chambers IR, Kane PJ. Signorini DF, et al. Bilateral ICP Monitoring: Its Importance in Detecting The Severity of Secondary Insults. Acta Neurochir. Suppl. 1998; 71: 42-43.
- Chapman Ph., Cosman Er., ARNOLD MA. The Relationship Between Ventricular Fluid Pressure and Body Position in Normal Subjects and Subjects with Shunts: A Telemetric Study. Neurrosurgery 1990; 26: 181-189.
- COHADON F. ET AL. Physiology of Intracranial Pressure. General Physiopathology of Intracranial Hypertensions. Neurochirirgie 1974; 20 (6): 489 - 520.
- Cremer Ol., Van Dijk GW., Van Wensen E. Effect of Intracranial Pressure Monitoring and Targeted Intensive Care on Functional Outcome After Severe Head Injury. Crit. Care Med. 2005; 33: 2207 - 2213.
- Czosnyka M. and Pickard JD. Monitoring and Interpretation of Intracranial Pressure. J. Neurol. Neurrosurg. Psychiatry 2004; 75: 813 - 821.
- Czosnyka M, Brady K, Reinhard M, et al. Monitoring of Cerebrovascular Autoregulation: Facts, Myths, and Missing Links. Neuroccrit. Care. 2009; 10 (3): 373-86.
- Czosnyka M, Matta B, Smielewski P. Cerebral Perfusion Pressure in Head-Injured Patients: A NonInvasive Assessment Using Transcranial Doppler Ultrasonography. J. Neurrosurg. 1998; 88: 802 - 808.
- DAVSON H, HOLLINGSWORTH G, SEGAL MB. The Mechanism of Drainage Of The Cerebrospinal Fluid. Brain 1970; 93: 665 - 678.
- Davson H. Physiology of The Cerbrospinal Fluid. Edinburg: churchill; 1967.
- Davson NH, Welch K, Segal MB. The Physiology and Pathophysiology of Cerebrospinal Fluid. New York: Churchill Livingstone; 1987.
- Dunn LT. Raised Intracranial Pressure. J Neurol. Neurrosurg. Psychiatry 2002; 73 (1): 23-27.
- Ecker H. Irregular Fluctuation on Elevated Cerebrospinal Fluid Pressure. Such Fluctuations As a Measure of Dysfunction of Cerebrovascular Episodes, Pseudotumor Cerebri and Head Injury. Arch. Neurol. Psychiatry 1955; 74: 641-649.
- EIDE P.K. A New Method for Processing of Continuous Intracranial Pressure Signals. MED EG PHYSICS 2006; 28: 579-587.
- Fichtner J, Güresir E, Seifert V, Raabe A. Efficacy of Silver-Bearing External Ventricular Drainage Catheters: A Retrospective Analysis. J neurrosurg. 2009.
- Ghajar J. Intracranial Pressure Monitoring Techniques. NEW HORIZ. 1995; 3 (3): 395-339.
- Grande Po, Asgeirssson B, Nordstrom C. Aspects on the Cerebral Perfusion Pressure During Therapy of a Traumatic Head Injury. Acta Anaesthesiol. 1997; 110: 36 - 40.
- Greenberg MS. Handbook of Neurrosurgery. Fifth Edition. NEW YORK: Thieme; 2001.
- Guillaume J, Janny P. Manometrient Interacranienne Continué Interest De La Methode Et Premiers Resultants. Rev. Neurol. 1951; 84: 131 - 142.
- Janny P. La Pression Intra-Cranielle Chez L`home. These (1950). Aubire: Clermont-Reproduction 1972.Continuous Recording and Control of Ventricular Fluid Pressure in Neurrosurgical Practice. ACTA PSYCHIAT. KBH. 1960; 149: 193.
- Jonston H.I., Rowan J.O.: Raised Intracranial Pressure and Cerebral Blood Flow.3.Venous Outflow Tract Pressure and Vascular Resistance In Experimental Intracranial Hyperantsion. J.neurol. Neurrosurg. Psychiatry 1974; 37: 392-402.
- Keays RT, Alexander GJ, Williams R. The Safety and Value of Extradural Intracranial Pressure Monitors in Fulminant Hepatic Failure. J. Hepatol. 1993; 18: 205-209.
- Koshkinen Lo, OliveCrona M. Clinical Experience with the Intraparenchymal Intracranial Pressure Monitoring Codman MicroSensor System. Neurrosurgery 2005; 56: 693 - 698.
- Langfitt TW, Weinstein JD, Kassell NF, et al. TRANSMISSION OF INCRASED INTRACRANIAL PRESSURE I. WITHIN THE CRANIOSPINAL AXIS. J. Neurrosurg 1964; 21 (11): 989 - 997.
- Lundberg N. Continuous Recording and Control of Ventricular Fluid Pressure in Neurrosurgical Practice. ACTA PSYCHIAT. KBH. 1960; 149: 193.
- Marion D.W., Spiegel T.P. Changes in
The need for treatment of hypertension is experiencing up to 40% of the population of Russia and Ukraine. These are people who have blood pressure exceed 140/90. Our countries have the highest mortality rate from cardiovascular diseases in Europe. Unfortunately, no more than 15% of patients with hypertension are obtained. This is due to the fact that most people with elevated blood pressure do not even suspect their problem. If the hypertensive disease is not treated, then the patient has the risk of death from heart attack, stroke or kidney failure, and the life expectancy is reduced by 5-10 years. Therefore, examine information about the treatment of hypertension, which are presented on our website, at least for prevention. Here you will find out everything you need to normalize your blood pressure and extend the active life:
- Hypertensive crisis: prevention and emergency assistance;
- How to choose an inexpensive and high-quality tonometer to measure the pressure on your own and relatives;
- How to reduce blood pressure using a properly selected diet, without using drugs;
- Efficient and safe treatment of arterial hypertension with vitamins and minerals;
- As doctors help bring blood pressure to the norm by special groups of patients: elderly people and pregnant women.
Is it possible to normalize arterial pressure by folk remedies?
Various herbal fees have long been used for arterial hypertension. They stimulate the protective forces of the body, saturate by it with vitamins, but do not have a significant effect to reduce blood pressure. It should be recognized that the treatment of hypertensive disease by folk remedies is rather "distracting" measures. At the initial stage, they can benefit, but only in combination with diet and exercise. If you have hypertension 2 or more than 3 degrees - without serious drugs do not do! At this stage of the disease, the use of folk agents instead of drugs often lead patients to hospital with stroke, infarction or kidney failure, and even straight on the cemetery. Nevertheless, it is proved that garlic use is beneficial with elevated pressure and cardiovascular diseases. Also on our site there are unique materials that will teach you how to quickly and effectively get rid of pressure problems with the help of vitamins and minerals, without the "chemical" drugs.
- Hypertensive disease: People's way to recover from it on 1 and 2 stages
- Garlic - folk remedy for hypertension
- Soothing herbal teas to reduce pressure
Typical complications of hypertensive disease are:
- Cardiovascular disease
- Kidney defeat
- Brain circulation disorders
- Worsening vision
If you have increased blood pressure already led to one or another complications, then in this case the purpose of drugs has its own characteristics. For people who have suffered a stroke or infarction, there is their own treatment tactics. Patients whose kidney problems or with vision are treated differently.
Who is in the risk group of hypertensive disease
Arterial hypertension rarely develops in people younger than 30 years. If a young man has a blood pressure is steady, then this is a true sign of the presence of a serious illness: most likely the defeat of the kidneys or adrenal glands. Risk factors for the development of hypertension and cardiovascular disorders in middle-aged people:
- Obesity
- Smoking
- Frequent stresses at work or in the family
- Bad blood test indicators for cholesterol: too much "bad" cholesterol and little "good".
While hypertension proceeds at the initial stage, i.e. blood pressure is increased no more than 160/100 mm. RT. Art., This dangerous disease is rarely diagnosed by changes in the patient's well-being. This is because the disease develops gradually, and the body has time to adapt. During this period, patients are generally lacking any symptoms in general. However, at the level of arterial pressure 140/90 - 160/100 mm. RT. Art. Domestic organs are already working with an increased load. Because of this, they are "wearing" faster. The risk increases that some of the livelihood systems of the body will suddenly give a "failure".
Is it possible to cure hypertension without giving up the joys of life?
Why are measures that usually recommend doctors so rarely help? Because the advice of doctors is most often too difficult to fulfill in real life. Doctors recommend patients to voluntarily abandon most of the joys of their life. Naturally, patients are not too hurry to do it.
It is good if the hypertone is daily disciplined to swallow the pills that will be prescribed. At best, for several years, he will delay the attack of the defeat of target organs. But, as a rule, infarction or stroke still do not have to wait too long. Please note that for the state it is actually profitable because the number of pensioners decreases, as well as the period during which they have to pay pensions. What to do? Is there any effective way to take blood pressure under control and extend life? It turns out there. Moreover, this wonderful way does not bring suffering to patients, rather, even on the contrary. So, we set and checked on dozens of patients that the best method of treatment of hypertension is a limitation of carbohydrates in the diet. Low-carbohydrate diet helps almost 100% of patients with hypertension, in which this disease is combined with obesity or type 2 diabetes. 
- The best way to recover from hypertension (quickly, easy, useful for health, without "chemical" drugs and bids)
- Do you have hypertension + insomnia + irritability? This is a magnesium deficiency in the body!
- Hypertension, its causes and how you can eliminate them
It turns out that you can eat meat, fish, oily bird, eggs, butter, etc. - and have a normal blood pressure of about 120-130 / 80, as well as a great level of cholesterol in the blood. Many patients first do not believe that it is possible because it seems too good. Nevertheless, it is true. A few weeks later, you yourself make sure that you can eat delicious and satisfying, and at the same time blood pressure is normalized. Test blood tests to cholesterol - and you will see that its performance is also improved. So, the "new life" can be safely continued. Since on a low-carbohydrate diet you will feel full and satisfied all the time, it will not be reasons to "break down" and return to the old power regime.  Low-carbohydrate diets (Duucan, Kremlin and Atkins) triumphantly walk around the country, despite the desperate resistance of the "official" medicine. The most benefit they bring people suffering:
Low-carbohydrate diets (Duucan, Kremlin and Atkins) triumphantly walk around the country, despite the desperate resistance of the "official" medicine. The most benefit they bring people suffering:
- obesity
- type 2 diabetes
- epilepsy.
- ... well, and at the same time quickly normalize blood pressure.
Why do the doctors continue to promote these diets? Because they are losses in millions of dollars for drug manufacturers, and many doctors will soon leave without work. But for patients, this is an excellent opportunity to extend your life and free yourself from heavy ailments. Attention! This method is not suitable if you have a "secondary" hypertension that some other "primary" disease caused. For example, progressive renal failure or tumor of adrenal glands. In such cases, hypertension is not amenable to conventional treatment. It will pass only when the doctor determines and cure the primary disease. This concerns no more than 5-10% of patients from their total number. If you already have renal failure, problems with the liver or serious diseases of the gastrointestinal tract - to apply only in coordination with the doctor and under its careful control. The restriction of carbohydrates in the diet is not recommended for pregnant women.
Pressure medications: Take only if without them no longer do
At the initial stage of the disease, it is often possible to normalize arterial pressure only by moving to a healthy lifestyle. And only if such attempts are unsuccessful, then you have to take medicines from hypertension, which, without exception, have side effects. Nevertheless, drugs reduce the risk of formidable complications of hypertension. Our site presents all the necessary information about drugs that are prescribed if blood pressure is greatly improved and "to knock down" in a different way. After reading our articles about hypotonic (reduced pressure) drugs, you will become an "informed patient" and will be able to effectively cooperate with your doctor who will choose a pill for you. Do you know about combined drugs from high pressure? These are medicines that contain at the same time two or even three actors from different classes of hypotensive drugs. Their use often reduces the dosage and increase the effectiveness of treatment. In many cases, medicines from hypertension from various groups neutralize side effects of each other.
- Treatment of hypertension with combined drugs
- What are the medicines from hypertension: full review
- List of medicines from hypertension - titles, descriptions of drugs
- Medicines for the treatment of hypertensive crisis
 You, most likely, did not know that, but doctors consider any good blood pressure, if it is able to reduce the risk of hypertension complications (infarction, stroke or kidney damage) at least 25%. If patients have a number of complications decrease by 30% - it means that the medication is generally remarkable. But does the "official" therapy arrange you, which has such low efficiency? If not, then read our article on how to get rid of hypertensive disease without drugs, with the help of vitamins and minerals.
You, most likely, did not know that, but doctors consider any good blood pressure, if it is able to reduce the risk of hypertension complications (infarction, stroke or kidney damage) at least 25%. If patients have a number of complications decrease by 30% - it means that the medication is generally remarkable. But does the "official" therapy arrange you, which has such low efficiency? If not, then read our article on how to get rid of hypertensive disease without drugs, with the help of vitamins and minerals.
Treatment of hypertension in the early stages without drugs
In the early stages of the disease, it is often possible to normalize arterial pressure using the patient's lifestyle correction without tablets.
|
Changes in a diet: |
|
But if your blood pressure is significantly increased, then the transition to a healthy lifestyle may not be enough to improve well-being. In this case, the doctor will appoint you a hypotensive (lower pressure) medicine. Unfortunately, all drugs from hypertension "are not only treated, but also cripples." Side effects of drugs for reducing blood pressure:
- fatigue,
- weakness,
- reduced potency
- sleep disorders
- raising the level of "bad" cholesterol in the blood
- and even heart attacks.
Therefore, the prevention of increased pressure in all respects is more profitable than the treatment of the disease. The best way of such prevention is: buy a good tonometer and regularly measure blood pressure yourself and all family members. We hope that this site will help to draw attention to the prevention and treatment of hypertension to reduce mortality from cardiovascular diseases. Be healthy, live long!
Essential hypertension: causes, symptoms, diagnosis, treatment, forecast
Essential hypertension is one of the most frequent diseases of the cardiovascular system, which has no geographical boundaries and is increasingly striking people of young age. The reasons for it still remain not fully solid, although risk factors and probable prerequisites are well known.
Primary, or essential, hypertension is a chronic increase in blood pressure, starting with an indicator of 140 mm Hg. Art. For systolic ("top") and 90 mm Hg. Art. For diastolic ("lower"). It is possible both an isolated increase in the first digit and the simultaneous increase in both.
On chronically elevated pressure and its danger in the form of a stroke, which it carries, did not hear the lazy. Nevertheless, not every person knows that the pressure "jumps," immediately goes to the doctor. Among the reached many, those who do not fulfill the prescriptions of specialists, does not accept medicines or grabs them when they overtake hypertensive crisis.
The lack of due attention to arterial pressure, non-permanent reception of drugs or rejection of treatment lead to a repeated increase in the risk of sharp vascular disasters in the brain, while maintaining blood pressure at the level of the norm, even with the help of drugs, not only improves well-being, but also prolongs Life vessels, heart and brain.
In the age of increased psycho-emotional loads and chronic stress, with deteriorating constantly environmental conditions, the lifestyle, nutrition is very important to monitor not only for individual symptoms that can talk about the launched stage of the disease, but also to regularly visit the doctor with the aim of prevention and early diagnosis of cunning hypertension. This applies, first of all, the people of the older generation, but also the young to the 30-35-year-old age also does not hurt.
Causes of primary hypertension
Essential arterial hypertension is called primary. This means that the specific reason in the form of organs of organs protruding blood pressure regulators was not found. It can be considered that the diagnosis of essential hypertension is a diagnosis of exclusion, when the surveys were confirmed that the pressure increases as if in itself, with healthy kidneys, a heart, an endocrine system (in contrast to the height of blood pressure during secondary hypertension).
However, it is not necessary to think that the reasons do not exist, and the pressure really fluctuates in itself. The accurate factor provoking hypertension is not formulated, but scientists called the conditions under which the disease develops. Today, primary hypertension is recognized as a multifactoric pathology, in the appearance of which the combination of various reasons is actively involved.

The most significant reasons for chronic long-term primary pressure increases are considered:
- Hereditary predisposition, which is confirmed by almost half of patients with essential hypertension;
- Overweight, increasing the risk of hypertension up to five times;
- Smoking, which also serves as a risk factor of ischemic changes in the heart;
- Low motor activity, often combined with overweight, which is quite natural;
- Features of nutrition - excess salt and fluid, lack of trace elements (magnesium, above all), vitamins, coffee abuse, tea, alcohol;
- Stress and psycho-emotional overload.
Traditionally, essential hypertension has recently relate to diseases of the elderly, but today the situation changes, an increasing number of patients with such a diagnosis have not been reached and 50 years. This says, above all, about the role of stress and lifestyle, rather than on the risk factors associated with age-related changes.
Among the unfavorable conditions that are at times increasing the risk of increase in pressure - diabetes mellitus, disorders of fat exchange, which are reflected in the lipidogram, an unhealthy lifestyle. Persons after 55 years are also very susceptible pathology.
Degrees and stage of primary hypertension
In order to more accurately judge the possible risks of the complications of hypertension, as well as to reflect the features of its flow, the degrees of pressure increases were calculated. The combination of the degree in accordance and numbers of pressure and certain risk factors, as well as related diseases, indicates the risk of hazardous complications - strokes, heart infarcates, acute renal or heart failure.
There are three degrees of essential hypertension:
- AG 1 degree when systolic pressure equals 140-159 mm Hg. Art., diastolic 90-99 mm RT. Art.
- At 2 degrees, pressure indicators are 160-179 and 100-109 mm RT, respectively. Art.
- 3 degree is the most severe when the pressure reaches 180/110 mm Hg. Art. and higher.
The diagnosis usually appears the degree, stage of the disease and the risk of complications. Thus, the degree is determined by the above mentioned parameters, while it is important not a single increase in pressure, but a constant, not less than three-four dimensions for a month.
The stage of primary hypertension is determined by characteristic symptoms and signs of involvement of internal organs. In the first stage there may be no symptoms and signs of changes in target organs, and only numbers on the tonometer speak about the presence of hypertension. At the second stage, changes in the walls of the vessels are progressing, some myocardial hypertrophy becomes noticeable, but these phenomena do not yet affect the activity of the heart and other organs. The third stage - it is also called the stage of organ changes - the signs of explicit vascular pathology and the work disorders of the target organs in connection with it.
Summing up the degree of essential hypertension, the risk factors and the features of the target bodies, the doctor easily determines the risk - insignificant, low, high, very high, determining the likelihood of deadly complications.
It is important to note that even the first extent of hypertension can be accompanied by a very high risk of complications in the presence of diabetes, lesions of target organs, combinations of more than three risk factors transferred in the past transient ischemic attacks or strokes. Patients with such aggravating factors should be extremely vigilant, even if the pressure "did not pass" for 140-149 mm Hg. Art.
A few words about targets
Blood pressure is an indicator of the enterprise, it affects not only the vessels and well-being, but also causes the defeat of various organs. Heart, kidneys, central nervous system, retina eye suffer. These organs are traditionally considered targets with essential hypertension.

The heart works with a large voltage, the result is myocardial hypertrophy. At the initial stages, hypertrophy provides adequate blood flow in the organs and is considered to be a mechanism for adapting to new conditions, and later the heart is depleted and lacking food. This circumstance explains the big tendency of patients with hypertension to heart attack, rhythm disorders, sudden coronary death.
Kidney is an important organ regulatory body. They are pretty much and suffer from its increase: sclerosis and dystrophy arterioles, the vascular loops of the gloms, are involved, the tubules are involved. With a large experience of hypertension, the likelihood of chronic renal failure is high, which is secondary to essential hypertension, but it aggravates it significantly.
The brain is experiencing a "cargo" of hypertension from the initial stages of the disease. Vascular changes lead to a violation of its nutrition, microinfarcts, nervous tissue dystrophy, and in the outcome - severe vascular dementia. With the brain lesion, most of the symptoms of pathology are associated - headache, noise in ears or head, reduction of memory and mental activity, etc. The hemorrhages and heart attacks are particularly dangerous against the background of hypertensive crises.
The retina is also considered a target organ. Its vessels acquire characteristic features, and the usual inspection of the Eye DNA in the first stage of hypertension can help in setting the correct diagnosis. Over time, the patient notes a decrease in vision, retinal retinal detachment is possible with significant pressure numbers.
Manifestations of essential hypertension
The main and the most first manifestation of essential arterial hypertension becomes exceeding the pressure indicators on the tonometer, fixed repeatedly. For a while, the patient lives with the initial hypertension and does not even notice her. This is understandable, because the vascular walls are not yet changed and able to control their tone and the width of the lumen, "adjusting" under the pressure numbers, therefore the symptoms may be absent. Some patients in this stage, even if there are some symptoms, do not give them due attention due to the apparent insignificance.

Excessive blood pressure only until time can flow asymptomatic. Gradually and inevitably changes the structure of vessels - arteries and arteriols first of all, the heart suffers. Without treatment, pathology acquires a clinically pronounced character, and in this stage the patient almost always hits the doctor.
At the initial stage, among the signs of disadvantage, patients note headaches, dizziness, weakness, possibly - noise in the ears, darkening in the eyes. These symptoms do not bother continuously, they occur periodically, often with strong physical or psycho-emotional loads, after errors in the diet.
Similar phenomena are not considered specific signs of hypertension, because they often happen in people with normal pressure, but it is still necessary to alert. The increase in headaches, their duration and intensity, the lack of effect from the usual analgesics should be the first reason for measuring the pressure of the house or appeal to the doctor.
In the second stage, the symptoms of pathology are becoming increasingly distinct, hypertensive crises are frequent with bright symptoms of increased pressure:
- Anxiety, redness of the face, sweating;
- Strong headache, a sense of pulsation in the head;
- Possible nausea and even vomiting;
- Feeling of pressure, chest pain, shortness of breath;
- Flushing flies in front of the eyes, darkening in the eyes.
These signs are most characteristic, but it happens that with relatively low pressure numbers, the patient has a strongest headache, apotal, pale. Often such crises accompany the tendencies to swells.
If the hypertensive crisis has been bought by drugs, then the patient continues its usual life, and not always paying due attention to the tonometer indicators and timely reception of drugs. If the diagnosis of essential hypertension is no longer in doubt, the crisis happened to repeatedly, then hope for spontaneous improvement or recovery is impossible - a disease is chronic, progressive, dangerous complications.
Gradually, an excess of blood pressure leads to changes in the internal organs, which is due, first of all, with a vascular factor. Vascular walls are the first to hit hypertension. For a while, it adapts to pressure fluctuations, then expanding its lumen, then reducing it to the desired diameter, but it cannot happen indefinitely.
The constant load contributes to irreversible changes up to sclerosis, when the walls of the arteries and arteriols become dense, brittle and incapable of a rapid reaction to pressure change. As a result, essential hypertension acquires a permanent nature, its degree increases, the risk becomes maximum.
In parallel with the vessels, adaptation to new conditions from the myocardium occurs. The heart pushes blood with more than normal, by force, the fibers are hypertrophy, the walls are thicken. With myocardial hypertrophy, you can link pain in the chest and the heart area, which appear in a number of patients as symptoms. At the later stages of the disease, the ischemia of the heart muscle is explicitly expressed, the coronary atherosclerosis is characteristic, angina symptoms arise, breaking the rhythm of the heart, the acute left-handhold insufficiency (pulmonary edema).
Persons with the third stage of essential hypertension have a number of signs from other bodies, which makes their complaints very diverse. Symptoms listed above are attached signs of vascular encephalopathy - a decrease in intellectual abilities, attention, memory, behavioral changes, a tendency to apathy or depression. Many patients have vision, its decline can be quickly progressive. Signs of heart failure grow, and the kidney defeat entails metabolism disorder (the increase in creatinine in the blood, the appearance of a protein in the urine, etc.).
Treatment of essential hypertension
The treatment of essential arterial hypertension is aimed at normalizing pressure, lifestyle and improving the function of target organs. It includes both drug therapy and general measures.
When the diagnosis is made, first of all, a lifestyle should be changed. Refusal of bad habits, changing the nature of nutrition, combating obesity and low motor activity - the first thing to be taken. In addition, these measures and the simplest, do not require hiking in the pharmacy and spending of large amounts of money.
Doctors The polyclinic is tirelessly spoken by the entire patient with essential hypertension on the need for a constant, systematic reception of drugs according to the recommended scheme. Despite this, many sick if they take pills, then periodically, when the disease will give themselves to be a hypertensive crisis.
In the case of essential hypertension, to postpone treatment or save on drugs is very dangerous. At any time, a critical increase in pressure with the most different consequences can happen, including fatally dangerous.

Medicase treatment of essential hypertension is appointed by a doctor. An independent reception of drugs is considered unacceptable, even if the tonometer showed hypertension, and the tablet proposed by a relative or a neighbor helps them. In the case of this disease, the success of treatment depends on the correctness of the appointed therapy, and this can be achieved only with a specialist.
Currently, approaches are adopted in the complex treatment of primary hypertension, when several drugs from different groups are appointed. Are used:
- Diuretic;
- ACE inhibitors;
- Calcium antagonists;
- Beta adrenoblocators;
- Angiotensin II receptor antagonists;
- Agonists of imidazoline receptors.
Preparations from each group have their own contraindications, therefore should be appointed only by a doctor based on the stage of the disease, response to treatment, concomitant background. At first, some one drug may be appointed in the form of monotherapy (an ACE inhibitor, as a rule), with an insufficient effect of the means of other groups add to it. This combination allows you to use drugs not at the maximum dose, thereby decreasing the likelihood of side effects.
ACE inhibitors are the most frequently used funds. Cappure is prescribed (effective in crisis), Enalapril, Lisinopil. These funds reduce the likelihood of complications, are well tolerated by patients and can be accepted for a long time. They are especially shown in cardiac and renal pathology, safe for admission in old age, during pregnancy, violations of carbohydrate and fat metabolism.
Angiotensin II receptor blockers (Losaryan, Valsartan) is one of the most modern groups of drugs from primary hypertension. They act selectively, therefore almost devoid of side effects. They are prescribed quite often, but the disadvantage can be the high cost.
Digensants are used to treat essential hypertension not one ten years old, but they do not lose their relevance. Hydrohlortiazide, Veroshapirius, Furosemid, ToramSamp, etc. are prescribed, and other diuretics are shown both for long-term reception and to relieve a hypertensive crisis. They can be part of combined hypotensive drugs together with drugs from other groups.
Calcium antagonists (amlodipine, diltiazene, verapamil) contribute to the relaxation of vascular walls, and spasm, as is well known, is the main link of pathogenesis of hypertension. They have advantages for patients with ischemic heart disease, rhythm disorders, expressed myocardial hypertrophy.
Beta-adrenobloclars (atenolol, metoprolol) not only reduce the pressure, but also reduce the load on myocardium, have an anesthetic effect during angina, normalize the heart rhythm, so they are usually prescribed during cardiac pathology - ischemic disease, tachyarimia, cardiosclerosis. Caution should be used in diabetes, obesity and other metabolic disorders.
Agonists of imidazoline receptors (Moxonidine) have a number of advantages compared to other means, among which they consider not only the lack of negative impact on metabolic processes, but also an improvement in them. Moxonidine is good with essential hypertension in patients with obesity, diabetes mellitus.
In addition to the listed groups, it is possible to appoint nootropic drugs in the symptoms of discirculatory hypertensive encephalopathy, vitamins and trace elements with changes in myocardium, sedatives at a high level of stress and emotional lability. The reception of plant extracts, tea with hypotensive properties is allowed, but it is not necessary to get involved in folk medicine - the treatment of herbs will not replace drug therapy appointed by the doctor.
The diagnosis of essential hypertension is not a sentence, and it is absolutely optionally it will end with a stroke or myocardial infarction. To prevent such a development of events, it is important to control the pressure of the house, periodically visit the doctor and be sure to take all the prescribed medicines, even if you have to do it for life. It is much easier to take a tablet than to fight with severe and very dangerous complications of hypertension.
Video: A series of lectures for arterial hypertension and its types
Effective methods for the treatment of hypertension iodine
Hypertension - the disease is cunning and dangerous. In the initial stage of symptoms, it is expressed sluggish, and many of us do not even suspect that they have already entered the multi-million rows of hypertensive.
So that this does not happen, hypertension must be kept in the ultrasound. For this, there are a lot of traditional methods associated with the systemic technique of hypotensive drugs, but today we will consider another option - the treatment of hypertension iodine.
It is used if the patient's body identified the lack of this element, and it became one of the causes of increased blood pressure. If the cause of hypertension lies in something else, then the pressure treatment with iodine does not raise the expected result.
Doctors have not yet disclosed the principle of exposure to iodine on the human body. But they proved that the lack of it can cause arrhythmia and bradycardia, manifest itself chronic fatigue and other characteristic reactions. Similar symptoms occur, and when the insufficiency of the function of the thyroid is diagnosed is a condition that often provokes an increase in blood pressure.
In our country, the deficiency of the iodine of varying degrees is observed in most of the population. The situation is better only in the seaside regions.
How to determine the lack of iodine in the body?
It is possible to test your body in a very simple way - to apply a mesh or other pattern to the skin on the skin, and then trace it with the dynamics. If the picture applied to the skin will disappear in 8 hours or per day, it will give reason to assume that the treatment of hypertension by iodine techniques can give a good result.
If during the day the test figure did not disappear and almost never brightened, it means that the speech deficit does not go, and apply the treatment of pressure by iodine on the Indian technique or by taking it inside.
How to treat iodine hypertension
Two types of people's iodine therapy are widely known and have many adherents:
- Indian method of treating hypertension iodine;
- Oral intake of iodine "tincture".
Indian hypertonium treatment with iodine
This ancient method is based on the introduction of the necessary element in the body of hypertensive through the skin in a strictly certain time - only two months a year - in March and September. When changing iodine administration, the Indian treatment diagram does not give effect.
And the second condition to achieve stabilization of the blood pressure - strictly observed in the treatment of hypertonium iodine scheme for applying an iodide solution on the body.
This is done like this:
- 1 day of the month - draw a line a little higher wrist of the left hand;
- 2 day. A similar line is applied over the ankle of the right leg;
- 3 number. We supply the right hand just above the wrist;
- 4 number. We apply a circular line over the ankle left leg;
- 5 day. We supply the iodine ring of a plot over the elbow of the left hand;
- 6 day. We apply a closed line over the knee of the right leg;
- 7 number. We repeat the action of the fifth day, but for the right hand;
- 8 day. Draw iodine Ring over the right knee;
- 9 number. Ask someone from the close to apply a solution with a solution on the back from the left shoulder to the opposite hip joint. It should only pass on the back, it is not necessary to clean it;
- 10 day. The same to do from the right shoulder towards the left thigh.
Then you should take a pause to the 21st, from which to conduct a re-course of Indian therapy. To achieve a persistent effect of stabilization of blood pressure, treatment must be carried out annually. The initial stage of hypertension as a result of such treatment can be in full. Heavy forms are better to be treated in close cooperation with the attending physician and under its control.
With a malignant course of hypertension, even with the improvement of the condition, it is impossible to completely cancel or reduce the dosage of the prescribed drugs. All changes in systematic traditional therapy must be coordinated with the doctor.
Iodine from hypertension can also be taken inward in the form of an alcohol solution or tinctures of aquatic or dairy. The alcohol solution in order to reduce the blood pressure is taken by small doses of a few drops, as a result of which atherosclerotic plaques on the walls of the vessels occur, the blood flow row is cleared. The walls of the vessels become more elastic, blood is diluted, the body resistance is growing towards infections.
Take inside and an aqueous solution of iodine, adding 10 drops into a glass of water. Use such "medicine" twice a day 30 minutes before meals. The healing course should continue exactly a month.
There are other methods of combating hypertension using oral administration of this element. Want to know how iodine with milk treat hypertension? There is also such a way - 15 drops of iodine add a slightly heated milk to a glass, drinking iodine milk should be 3 times a day after meals. The duration of treatment is also 30 days.
Reception of iodide tinctures is not suitable for everyone. This method is not suitable for people suffering from diseases of the gastrointestinal tract, pancreas and liver. Iodine, caught in the esophagus and stomach, annoying the mucous membrane and aggravates the unhealthy state of the person.
The use of compounds of this element inside may cause unpleasant side effects. It may be nausea and even vomiting, intestinal disorder and pain in the abdomen. Sometimes the side reaction to the reception of iodine is manifested by a darkening in the eyes, dizziness or even swelling of Queenka.
If the side effect is manifested by light symptoms and ailment, you need to stop the reception of the drug that caused them, and there is no unpleasant symptoms. In severe cases, urgent help of physicians may need.
It is especially important to quickly render it with the appearance of a quinque - a state that can end with a fatal outcome if the help does not sing in time.
Another risk that lifters those who are treated with iodine externally, - the appearance of burns when they are too abundant applying the solution on the skin. Sometimes such a burn is accompanied by severe pain, and this can cause a sharp increase in blood pressure under the influence of the stress factor.
The resulting burn must be thoroughly rinsed with clean running water, and then apply glucose as an antidote to glucose or a conventional toothpaste. After that, it is necessary to lubricate the scene of a burn with anyone under hand against the anti-grade composition.
Who can not be treated with iodine categorically
Iodine - harmless and harmless drug. But for some categories of people, its reception or even simply contact with the solution may be unsafe. For example, there are people who suffer from individual intolerance to this drug.
With the caustic and mandatory advice of the doctor to be treated with iodine in case of diseases such as tuberculosis, carpentry lesions of the skin. It is not recommended to treat in iodine of children using folk techniques. To refrain from such therapy implies women in a state of pregnancy or during the lactation period, as well as patients with hypoteriosis, receiving iodine-containing drugs.
No titleHealing becoming to normalize pressure from hypertensive and hypotonics.
Stava need time to normalize the process to harmoniously lead to a harmonious and comfortable state.
Therefore, becoming necessary to wear for a long time, and after the end of the work, the configured body will seek it yourself to support the result.I thank everyone separately for the help and diagnosis of Stava!
Attention! Becoming a new generation, which also affects the neuro-level, and still be on the tests !!
Therefore, there will not be enough tests and results, please only with experienced practices to use this becoming.
And invite experienced tests for tests !!Centre: Point - Otal - Raid - Sol - Kenaz - Yera Warraplanova
Left: zer. Naut - plastur - per. Laguz - Ar.
On right: Laguz - Berkana - Uruz - IngvazPoint - Operator
Otal - organism and blood system operator
Raid - on neuroorovna manages brain trunk and the development of JAM-1
Salt - normalizes the work of the circulatory system and heart
Kenaz - Energy to run the cure of hypertension and the help of a circulatory system
Yera Warraplanova - process engine and internal balance with external
zer. Naud- conscious need to normalize pressure
Plastur- Healing of the circulatory and hematopoietic system
per. Laguz - Exhale. Displays extra JAM-1 and other interfering normalization of matter
AR - results in a result - cure on the neurophysiological level.
Laguz - inhale. Health restoration flow in body
Uruz, Berkana, Ingvaz - Restoration of the physical bodyStar:
DRC from the moment of activation affecting the body normalizes the development of JAM1,
how much is needed for the chemical composition of blood at the moment for a comfortable
permanent condition of the body and for full-fledged work of blood and
the hematopoietic system as a whole, as well as lead the metabolism to the norm and displays
Surplus JAM-1 and other interfering normalization of the substance.
It works cyclically normalizing pressure and including when the pressure is deviated from the norm.Becoming working immediately in 3 directions:
- Neuroprogram. Normalization of the level of the JAM1 protein is its work out in the brain barrel.
- physi-program. Normalization of the hematopoietic and circulatory system, which leads to the complete cure of hypertension.
- bioprogram. Regeneration and improvement of metabolism in the bodyIntroduction for understanding:
The newest studies have found the cause of hypertension on the neurophysiological level,
What gave an explanation why any previously produced medicines did not heal, but only kept this disease.
So. Protein (protein) JAM-1 is produced in the brain barrel,
Regulates oxygen access to cells and binds leukocytes.
With a large concentration, attracts (attaching)
To endothelium (inner layer of blood vessels) leukocytes.
Which determines the level of pressure and access of oxygen to cells.
With artificial stimulation at a healthy experimental group only
Jam-1 protein, quickly obtained a resistant hypertension.
those. Driving JAM-1 and the center that produces it can be delivered from this disease.For good and health!
Migraine disease characterized by periodically repetitive bolts of headaches, usually in one half of the head. In this case, there are no serious injuries of the head, stroke, brain tumors, and the intensity and pulsating character of pain are binding to vascular headache, and not with a headache from voltage. Migraine headache is not associated with an increase in or a sharp decrease in blood pressure, a glaucoma attack or an increase in intracranial pressure (VCHD). Women are sick. In most cases, hereditary burden is noted; The disease often begins to manifest themselves during puberty. The mechanism of origin of headaches at M. is associated with changes in the tone of intra- and extra charge vessels; It is assumed that spasm develops first, and then a decrease in the tone of the vessels and as a result of which their abnormal expansion. The bouts of the headaches are combined with nausea, vomiting, light-andased. There is a pallor or redness of the skin of the face, grinding of brushes and stop, weakness, chills, yawning, etc. phenomena. Patients usually complain about the feeling of luminous sparks, zigzag lines, sometimes to reduce vision and fog in the eyes (Ophthalmic M.). In other cases, complaints arise on sensations of numbness, tingling in the limbs, sometimes represented and language. T.N. Symptomatic M. is a sign of organic diseases of the brain (tumors, vascular aneurysms, etc.).
Treatment: Normalization of vascular tone, soothing means
On this, I have created this formula.
The reservation is simple - (all according to the classics)
mid -
This Runic Vycle removes all the causes of the occurrence of a migraine attack, as well as removes the migraine attack itself, and the whole symptoms of migraine y (name).
End of a classic tissue. (This Runic Formula is valid until the result of the result)
Now foreseeing questions about the runes of which this work is connected.
Isa -Zerozka, suspended the development of an attack and give time to work the rest of the runes.
Dagaz - transforms the situation - the pain goes, + stabilizes the patient's condition, also stabilizes the pressure if the attack coincided with an attack of increasing or lowering pressure. Unfins in a pair with ISU.
Ingus is the restoration of the strength and balance of the body. Restores the energy system of the organism. The voltage and restores the balance, strengthens the general health condition.
Satal - to improve health.
Algiz - catches the bunch of an attack, cares all the symptoms and causes of the occurrence of an attack.
Gebo - all tightens in one point + establishes equilibrium in the body
Halgal - destroys everything that was torn by Gebo.
Naut - exemption from pain and problems that are accompanied by migraines.
EVAZ quickly makes changes.
Ansus for removing the shackles, including psychological
Berkana brings a noticeable relief + renewal of the elasticity of the vessels of the brain. + Gives restoration of the body after an attack.
Tours - starting push.
Kano - mitigation + highlighting problem areas in the body due to migraine.
Perto gives strength and includes additional resources for healing.
Riot - rapid results achievement.

Isa suspend pain syndrome.
Uruz accelerates the restoration of the forces after the disease, will help to feel updated. Range of vitality
EVAZ quickly make changes.
The yer will eliminate obstacles that prevent the results of the result. Give the opportunity to gain a "second breathing"
Wasya causes improved well-being. Independent physics.
Assault to remove the shackles, including psychological (such as subconscious anxiety or fear)
Berkana she helps to cope with women's problems and, in particular, brings a noticeable relief
Fall for liberation from problems associated with headache
Teivaz for quick recovery.
Soul for cure. Beneficially affects the general physical condition. And gives energy to work Stava.
One of the current "Runic Topics" is associated with questions how to choose a runery job, determine how correctly it is composed and whether it is suitable for solving one or another task.
It is believed that the shadow is an astral continuation of a person's personality (creatures), his image and silhouette. In fact, this is an unmanifested part, which relates to other worlds and is reflected in them.
Gumaglede.
Having become Gumaglede (the "joy of warriors") - a balanced energy, which satisfies the need for practice in energy and forces due to internal reserves and external sources. Runic Vych is a cipher in which "hidden" Icelandic runes and older feet.
So the new 2020 began. Let it be fruitful for you, generous for good news, interesting projects! Thank you that previous 12 months have you been with us. We appreciate your trust and desire for enlightenment, wisdom and gaining strength!
Complete the autumn gold with real fire with candles and they will help get rid of not only from Handra, send, give enlightenment, but also will be given in purification, strengthen protection and keep balance. .
They thought ... and decided to make a 15% discount in our ethno-shop first 15 buyers in July. Moreover, if we persuade (for example, by placing a wonderful post at home on the wall in social networks about our store - just report this through our communication form), then we will also apply a personal discount that can increase the already provided up to 20%. Interesting offer?
- Wrong wedding Ivan Krasko
- Dream interpretation: chain in a dream (shackles, dog on chains, jewelry)
- What dream dick (male body)?
- How to treat gout at home
- Dream Interpretation - Wolf: What dreams in a dream black, white, gray wolf?
- What dreams of a wolf: proper interpretation
- What dreams of a spoon and forks are taken if the cutlery is shot